A sprained ankle is one of the most common musculoskeletal injuries presenting to Sports Medicine Professionals the world over. So what is a sprained ankle, what structures are injured, what can you do in the early phases to manage the pain and swelling, how can you prevent ankle sprains and when do you need to see a Doctor or Physiotherapist for assessment, management advice and treatment?

What is a sprained ankle?
Put simply, a sprained ankle is a twisting or rotational injury which results in damage to the soft tissue structures of the ankle joint, this is the most common sports injury but there is lots of variability in terms of the mechanism, injured structures and interventions required to manage them.
An acute ankle sprain occurs with a sudden onset and is associated with both sporting and everyday activity. In a sporting context the injury may occur during a landing task, when changing direction or during a tackle whereas in the non-sporting injury it may occur due to uneven surfaces or simply slipping on a step or kerb!
Ankle sprains can occur during seemingly innocuous tasks and result in high levels of pain and swelling. The key is working out which are the severe sprain, moderate sprain, mild sprain injuries and what can be done to prevent further injury.

Types of ankle injury
Lateral ankle sprain
High ankle sprain
Deltoid ankle injury
Ankle fractures
Lateral ankle sprains
A lateral ankle sprain (inversion injury) most commonly occurs with a forced inversion and plantar flexion mechanism of injury. This twist of the ankle results in injury to the lateral ligaments primarily but may also include injury to the joint surface, the cartilage and the bone.
There are 3 primary lateral ligaments at the ankle joint:
Anterior Talofibular ligament (ATFL)
Calcaneofibular Ligament (CFL)
Posterior Talofibular ligament (PTFL)
Most ankle injuries regardless of severity are very painful when they occur. This makes it difficult to differentiate the most common ankle injuries which are a fairly mild ankle sprain from the less common multi-ligament severe sprain or fracture (broken bone). A Doctor or Physio can help determine if a fracture has occurred and will be guided by Ottawa ankle rules.
The injured ankle will usually become swollen instantly and it will be difficult to put the foot down due to pain and swelling or in more severe injury a feeling of instability or giving way.
Immediate Management of a sprained ankle injury
The Police Principle is a modern/modified first aid method of treating musculoskeletal injuries. https://www.physio-pedia.com/POLICE_Principle
POLICE is an acronym that stands for protection, optimal loading, ice compression, and elevation. It promotes and guides safe and effective loading in acute soft tissue injury management.
If your ankle sprain has just happened then we can follow this advice. Protect the injury by getting the foot off the ground if this is possible and limiting the range of motion , the optimal loading will come later but it is vitally important to apply ice to ease the pain and compression to limit the swelling, elevation will also help this.
Compression can be applied with an elastic bandage (such as tubigrip) or compressive ankle taping.
A chronic ankle sprain is one which recurrently is an issue. People will suffer acute on chronic episodes of the ankle giving way due to chronic ankle instability. This is usually a consequence of incomplete rehabilitation or returning to demanding tasks before giving the injured structures a chance to heal and for strengthening exercises to be effective. To reduce the risk of a future ankle sprain it is important to get appropriate advice and Physiotherapy (Physical Therapy) input.
The ankle may benefit from a period of immobilisation. This can be in the form of an ankle brace, a more restrictive Orthopaedic Boot or with the use of crutches in combination with immobilisation to protect the injured structures in the early phases post-injury.

It is likely that range of motion will be impacted by pain and swelling but in the cases of ankle brace and boot both can be removed to allow gentle Range of motion (ROM) exercises which will help with swelling and reduce the impact of muscle wasting and joint stiffness.
How do I know if my ankle pain is serious?
With most ankle injuries it will be important to get professional advice in order to diagnose and determine the injury severity . This diagnosis will be through a combination of clinical assessment and if indicated, X-Ray or MRI scan. If a severe ankle sprain is suspected then a visit to A&E would be recommended to rule out a fracture.
Grade 1 – With a grade 1 ligament injury the ankle is likely to be painful and swollen but won’t be unstable. This is because the ligament has been stretched and will be oedematous but the actual ligament fibres haven’t torn. In grade 1 injury, usually only one ligament is involved and it is primarily the ATFL.
Grade 2 – With a grade 2 ligament injury there will be a partial tear in the ligament fibers. This will result in more extensive swelling and bruising. In terms of ankle stability the ankle may feel unstable especially if more than one of the ankle ligaments is involved.
Grade 3 – With a grade 3 ligament injury there has been a complete tear of the ligament. This may include a single ligament of in the case of severe ankle sprains two or three ligaments may be involved to varying degrees. The ankle will feel unstable.
High ankle sprain
A high ankle sprain (also known as a syndesmosis injury) is discussed in greater detail in a previous blog (read it here) however the basic principles of management will be discussed here.
High ankle sprains occur during rotational mechanisms of injury and often involve the foot getting caught in something. In a sporting setting, this can be in a tackle in football or when the foot is caught beneath the scrum in rugby. In day-to-day activity, it can also occur when stepping from a height or getting the lower limb twisted under you during a fall.
The most extreme version of a high ankle sprain will actually progress to a bone injury or fracture when the rotational forces are high enough to result in a fractured fibula, in most cases involving just soft tissues of the lower limb it will be the ligaments which in effect hold the distal ends of the shin bones together which are injured.
These often injured structures in the case of high ankle sprains include
Anterior Inferior Tibiofibula Ligament (AITFL)
Posterior Inferior Tibiofibula Ligament (PITFL)
Interosseous Ligament (IOL)
Interosseous Membrane (IM)
These ligaments and membrane structures provide a fibrous soft tissue mortise joint at the distal end of the Tibia and Fibula which the Talus sits into and collectively are known as the Syndesmosis. Previously these structures were often missed at initial diagnosis as they often don’t present as painfully as a lateral ligament injury and tend to swell less. This lesser pain and swelling can be misleading and often resulted in people returning to high-level activity too soon with resultant re-injury.
From a functional perspective, the ligaments of the syndesmosis are of course closely connected with the lateral and medial ligaments of the ankle and an injury to the syndesmosis will often involve some of or all of the medial (Deltoid) or lateral (especially ATFL) ligaments.
How severe is my High Ankle (Syndesmosis) Injury
Sikka grading –
Grade 1 – isolated injury to the AITFL.
Grade 2 – injury to the AITFL and IL.
Grade 3 – injury to the AITFL, IL and PITFL.
Grade 4 – injury to the AITFL, IL, PITFL and deltoid ligament.
Clinical grading –
Grade I: Involves injury to the anterior deltoid ligament and the distal IL but without tearing of the more proximal syndesmosis or the deep deltoid ligament. The AITFL is often very tender to palpation and may have a higher-grade injury; because no diastasis is present, the injury is, by definition, stable.
Grade II: involves disruption of the anterior and deep deltoid ligaments as well as a tear in a significant portion of the syndesmosis, resulting in a POTENTIALLY unstable ankle that is still normally aligned on non-stress radiographs. This poses particular diagnostic challenges, because the extent of the injury and its occult instability are often more difficult to recognise (see below for Grade 2A v 2B decision-making).
Grade III: Involves severe external rotation and abduction, with complete disruption of the medial ligaments and extensive disruption of the syndesmosis, frequently accompanied by fracture of the proximal fibula. Such injuries are overtly unstable on initial examination and standard radiographs.
Treatment for ankle sprains
It’s important to note that the vast majority of ankle sprains heal well with quite simple management. It is very rare that surgery will be required though you may on occasion see orthopaedic surgeons to be sure that a reconstruction of the injured ligaments isn’t required.
The sooner you get advice from Sports medicine specialists the easier it is to manage these injuries. Simple measures taken in the first days and weeks after injury can have hugely beneficial impact on things like swelling, muscle strength, joint range of motion and pain. Severe injuries which are managed conservatively may require a longer immobilisation period but ultimately rehabilitation will look the same. The aim being to get the injured structures strong, stable and able to cope with the demands of the individual’s life or sport.
An injured foot and ankle can impact on the most basic of tasks but with a complete rehabilitation program, recovery can be expected in 3-4 weeks for a mild injury. The key is to maintain good muscle strength so as not to become a recurrent sprainer and fall into the trap of believing you have weak ankles.
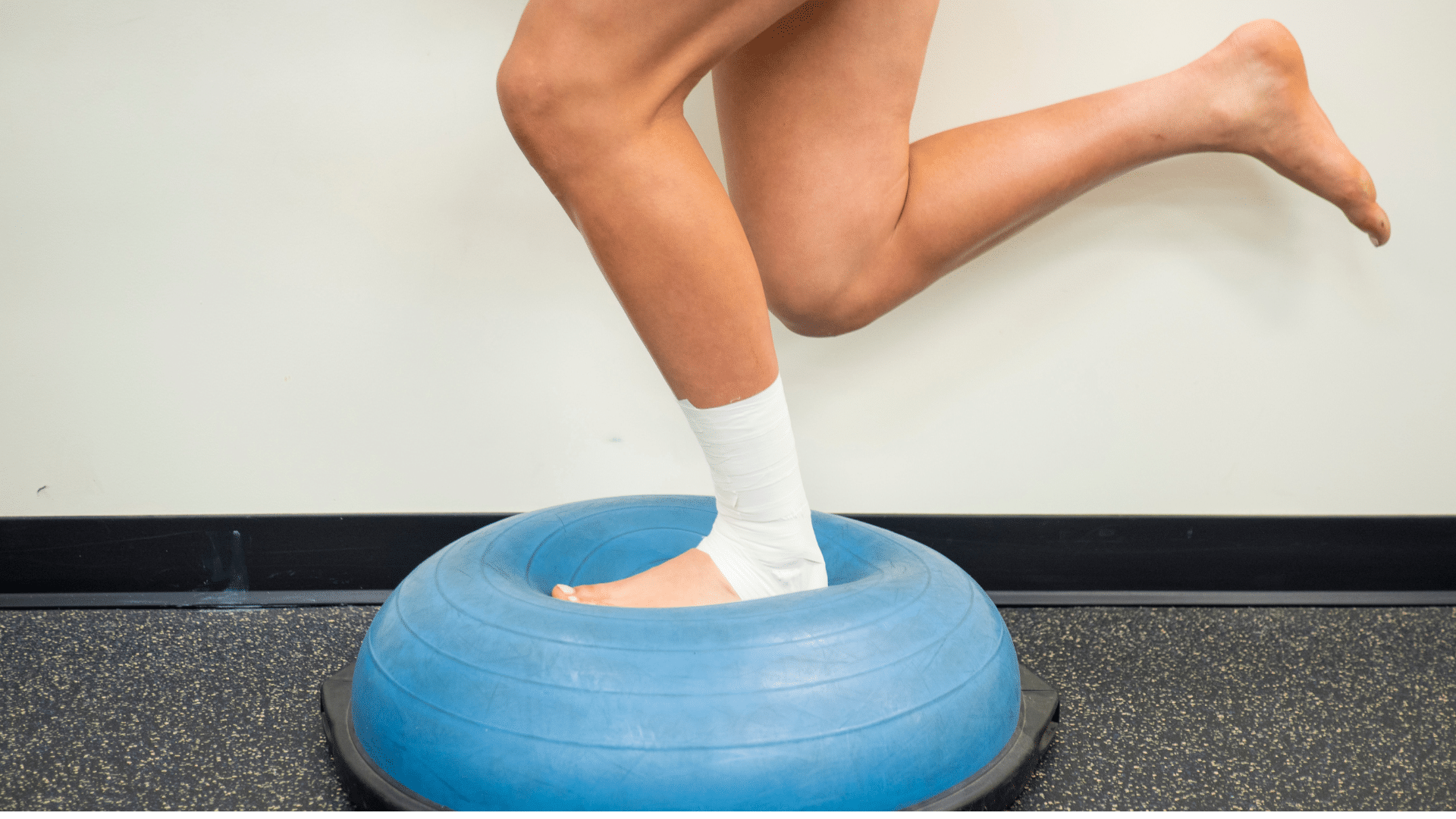
Whilst some people can have a functional instability this can usually be improved with appropriate strengthening exercises, balance (proprioception) exercises and jump – land (plyometric) tasks.
Prevention of ankle injuries
For those involved in sporting activity which involves contact, change of direction and jumping it is vital the athletic development program running alongside the technical training program is designed to create robustness in tasks which can result in ankle ligament injury. Prevention of ankle injury exercises should be incorporated into gym and pitch or court based training programs to reduce the risk of injury whilst accepting it is impossible to prevent every injury. The FIFA 11+ is an example of a simple program which individuals and groups can do.
Summary of ankle injuries
The majority of ankle injuries are mild to moderate in severity and can be managed with appropriate treatment and exercise modalities. Rehabilitation should be carried out under the guidance of a Sports and exercise medicine consultant or Physiotherapist specialised in sports injuries to achieve optimal outcomes. Here at R4P we believe in rehabilitation back to performance and treat the general public and athletic population with the same level of detail, care and expertise. If you are unsure about what steps to take next with acute, recurrent or chronic ankle sprains get in touch and we will help in any way we can.